+91 8080571771

Fluoride has a unique ability to strengthen enamel. Enamel, the hardest substance in nature is made up of an incredible crystalline substance called calcium hydroxyapatite. When fluoride is incorporated into the enamel it becomes calcium fluorapatite, which is much more resistant to acid attack (decay).
It also reverses the early decay. In children under 6 years of age fluoride becomes incorporated into the development of the permanent teeth, making it difficult for acids to de-mineralize the teeth. Fluoride varnish should be applied at least twice yearly in all children. Fluoride varnish is a pale yellow gel that sets quickly when applied to children’s teeth using a soft brush. The varnish sets quickly, has a pleasant taste and a fruity smell. It is certainly important for infants and children between the ages of 6 months and 16 years to be exposed to fluoride. this the time-frame during which the primary and permanent teeth come in. Are there any risks? However, the risk of developing white spots as a result of fluoride varnish is very small. After the application the fluoride varnish should remain on the child's teeth for the rest of the day and also overnight to provide the most benefit.
Please make sure :
you do not brush your child's teeth tonight, but from tomorrow morning brush them at least twice daily, in the morning and last thing at night using toothpaste containing at least 1000 - 1500 ppm (parts per million) fluoride.The last and most important factor to consider: Trust your dentist — your dentist will know your child's risk for decay, will monitor your child's teeth and other factors like diet, dental plaque control (how well you remove acid producing bacteria), seal the surfaces that decay where the toothbrush can't reach.
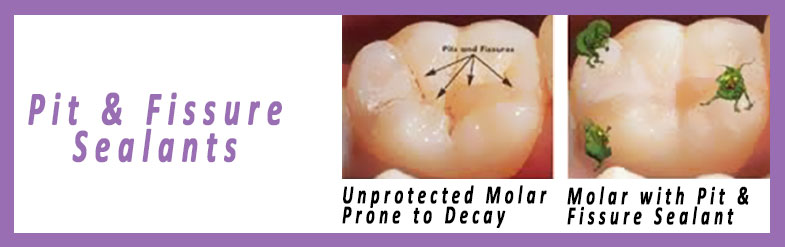
Kid’s teeth are often groovy. There are two types of grooves that may be found in the biting surface of teeth, known as pits and fissures. As the name suggests, pits are small indentations (pits) in the tooth’s dental enamel (the hard covering which protects the tooth from bacteria and other nasties).
Fissures are the grooves which form naturally and give shape and texture to the biting surface of 'chewing' teeth at the back of the mouth (called molars and premolars). They typically only affect the 'chewing' teeth, but in a minority of exceptionally groovy children the 'biting' teeth at the front of the mouth (called canines and incisors) may also have fissures. No matter how thoroughly your child cleans and flosses their teeth, completely removing bacteria and other nasties from fissures is impossible if the grooves are too narrow. Thankfully dentists have developed pit and fissure sealants which can fill and seal the grooves in children’s teeth and prevent bacteria getting in. They make teeth easier to clean and reduce the risk a child will experience tooth decay. Fissure sealants are recommended for filling the adult or primary teeth of children who have a high risk of developing cavities. Dental cavities are five times more likely to occur in pits and fissures. Teeth protected with fissure sealants are 22 times less likely to decay than unprotected teeth. Now those are good odds, but only around 20% of children have fissure sealants. Dentists believe that if sealants were more common, tooth decay in children would be less common.
Fissure sealants made from materials called glass ionomer cement or composite resin can be used to seal up these pesky grooves. The sealants form a mechanical barrier which prevents bacteria and other nasties entering the grooves and considerably reduces the likelihood of cavities forming in the grooves. As a general rule, they’re recommended for filling the molars of kids with a high risk of tooth decay, such as those who have already had a couple of dental cavities filled and those who lack fluoride in their drinking water. The fissure sealants only take about 10 minutes to put in place and can be applied by a dentist, dental therapist or dental hygienist. To place the sealant, your child’s dentist will clean the tooth to ensure there are no particles of food or other contaminants stuck to it and then dry it thoroughly, as the sealant can only stick properly to a tooth that is perfectly clean and dry. Then the sealant is added to fill the grooves and keep food particles and bacteria out. The sealant is allowed to dry, until it is hard and durable. Sometimes the dentist will shine a strong light on the sealant to help it set. Your child’s bite will be checked, and if the sealant has affected the way your child’s teeth press together, it may be necessary to polish away tiny amounts of the sealant to correct this. They are easy and fast for your child’s dentist to put in place, and typically last a long time.It’s important to remember that fissure sealants are not a magic solution to tooth decay. They are just one part of a multi-dimensional dental hygiene routine which should involve brushing and flossing, regular trips to the dentist and avoidance of foods which promote tooth decay. Remember that fissure sealants are not a magic solution to tooth decay. Ensure that your child continues to brush and floss regularly once their fissure sealants have been put in place.
Ensure your children avoid foods which promote tooth decay such as sweets and sugary drinks.Dental sealants are recognized as an effective approach to preventing pit and fissure caries in children.

Dental caries is a dynamic process that involves a susceptible tooth, cariogenic bacteria in dental plaque (streptococcus mutans and lactobacillus), and a fermentable carbohydrate. However, all simple sugars are potentially cariogenic. Sugary foods or liquids consumed 20 minutes apart allows for separate opportunities for bacteria to feed and produce acid. When the pH of the dental plaque falls below 5.5, the caries process begins. Form and composition of a fermentable carbohydrate plays a secondary role depending on how long it takes for a food or drink to clear the oral cavity. Liquids clear faster than soft, sticky foods. Regular dental check-ups can help detect and monitor potential problems.
Destructive effects of soda, juice, and the popular energy drinks are a major cause of early childhood caries and decay among both children and teenagers, Diet soda and energy drinks includes both citric and phosphoric acid, which may cause direct demineralization of the tooth enamel. Rinsing the mouth with water, bypassing the teeth by using a straw, chewing gum with xylitol, and consuming the potential caries causing drinks with a meal can help reduce the negative effects of liquid fermentable carbohydrates.
Protective factors from specific foods and diet sequencing may also be utilized in order to reduce the destructive influence of fermentable carbohydrates. Fats and proteins consumed in a meal help coat the tooth surface to protect it from sugars. Consuming dairy products keeps the saliva rich in calcium and phosphorus, offering benefits of remineralization by preventing the pH of the mouth falling below 5.5. Fluoride in both food and water will also help remineralize the enamel. Dietary advice should be formulated which is both realistic and positive. Trying to dissuade children from consuming products, which they perceive to be tasty and pleasurable is counter productive and more emphasis should be given to tooth brushing using a fluoride toothpaste. They initiate a sticky film, known as dental plaque, on the surface of the tooth. Bacteria in dental plaque use fermentable carbohydrates to form acids. Fermentable carbohydrates are sugars and other carbohydrates from food and drink that can be fermented by bacteria. The acids formed dissolve minerals such as calcium and phosphate from the tooth. This is called demineralisation.
But tooth decay is not inevitable. Saliva clears food debris from the mouth, neutralises acids produced from plaque bacteria and provides calcium and phosphate to the teeth in a process called remineralisation. Saliva also acts as a reservoir for fluorides from toothpaste or from fluoridated water. Fluoride helps control dental caries by remineralising the teeth and inhibiting bacterial acid production, which reduces or slows the decay process.Although the decline in tooth decay in many countries has been largely linked to fluoride exposure and improved dental hygiene, eating habits still affect the risk of tooth decay.
[A] Fermentable Carbohydrates :
For many years the simplified message to prevent tooth decay was don't eat too much sugar and sugary food's. Over the last few decades sugar intake in many countries has remained constant whilst caries levels have declined. This suggests that where appropriate oral hygiene is practised (i.e. regular tooth brushing using fluoride toothpaste) the role of sugars in tooth decay is less manifest.
Advice to replace sugar with starchy foods to avoid tooth decay is of questionable value. It is now known that any food containing fermentable carbohydrates can contribute to tooth decay. This means that as well as sweets and confectionery, pasta, rice, potato crisps, fruits, and even bread can set the scene for demineralisation.
[B] Food Characteristics :
The physical characteristics of a food, particularly how much it clings to the teeth also influence the tooth decay equation. Foods that adhere to the teeth increase the risk of tooth decay compared to foods that clear from the mouth quickly. For example crisps and biscuits stick to teeth for longer periods than foods such as caramels and jelly beans. This may be because caramels and jelly-beans contain soluble sugars that are washed away more quickly by saliva. The longer carbohydrate-containing foods are around the teeth, the more time bacteria have to produce acid and the greater the chance of demineralisation.
[C] Frequency of Eating :
The frequency of sugar eaten is the primary factor involved in the caries process. Each time we nibble a food or sip a drink containing carbohydrates, any decay-causing bacteria present on the teeth start to produce acid and demineralisation commences. This continues for 20 to 30 minutes after eating or drinking, longer if food debris is locally entrapped or remains in the mouth. In between periods of eating and drinking saliva works to neutralise the acids and assist in the process of remineralisation. If food or drink is taken too frequently the tooth enamel does not have a chance to remineralise completely and caries can start to occur. This is why nibbling or sipping continuously throughout the day should be discouraged. The best advice is to limit the consumption of food and drink containing carbohydrates to no more than 6 occasions per day and ensure teeth are brushed with fluoride toothpaste twice a day.
Baby bottle caries or nursing caries is a condition in which infant's teeth are damaged by prolonged frequent exposure to drinks containing sugars usually via a baby feeding bottle. In particular, problems arise when infants are put to sleep with a bottle of milk or juice. The flow of saliva is greatly reduced during sleep and the sweet liquid pools around the teeth for extended periods of time. This provides the perfect environment for tooth decay to develop.
[D] Protective Foods :
Some foods help protect against tooth decay. For example hard cheese increases the flow of saliva. Cheese also contains calcium, phosphate and casein, a milk protein, which protects against demineralisation. Finishing a meal with a piece of cheese helps counteract acids produced from carbohydrate foods eaten at the same meal. Milk also contains calcium, phosphate and casein, and the milk sugar, lactose, is less cariogenic (caries causing) than other sugars. Nevertheless caries have been found in children breastfed frequently on demand.